Risks include patient-related factors (e.g. underlying disease), external factors (e.g. nicotine consumption) and technical errors when closing the abdominal wall. An incisional hernia should be closed at the latest when the patient has symptoms.
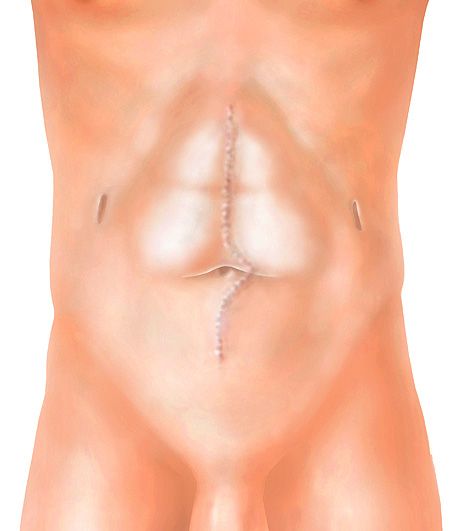
Every scar in the abdominal wall is a weak point. This is why an incisional hernia develops in about one fifth of patients.
Risks include patient-related factors (e.g. underlying disease), external factors (e.g. nicotine consumption) and technical errors when closing the abdominal wall. An incisional hernia should be closed at the latest when the patient has symptoms.
The choice of technique depends on various factors such as previous operations, the number and distribution of hernias, other hernias present at the same time and the patient’s wishes. The operation is planned individually. The closure of the hernia is almost always reinforced with a mesh insert. In order to avoid recurring hernias, we use large meshes that cover the entire existing scar. In order to achieve a pleasing cosmetic result, we perform the operation together with plastic surgery colleagues if necessary.
Open surgery is usually performed by inserting a mesh in front of the peritoneum. Either a transverse incision is made in the lower abdomen with possible correction of a fat apron. The abdominal wall is then opened and the peritoneum is detached from the abdominal wall. The mesh of the required size is inserted and fixed into the space created in this way and the abdominal wall is closed over it.
For laparoscopic intraperitoneal mesh insertion, air is first insufflated into the abdominal cavity to enable work to be carried out using a camera and special instruments. The hernia is then closed with a plastic mesh specially developed for this operation.
Attending Physician, Department of Visceral Surgery and Transplantation
As a patient, you cannot register directly for a consultation. Please get a referral from your primary care physician, specialist.
Easily assign your patient online.