Diverticular disease - what you can do yourself
The following tips help with diverticular disease and can improve existing symptoms:
- Healthy and balanced diet: Consume as much fiber as possible, which is good for digestion. Wholemeal products, fruit, vegetables and pulses are particularly good sources of fiber. You can also include nuts, grains or seeds in your diet if you have diverticulitis. Contrary to previous assumptions, they do not pose any particular risk. Whether the consumption of probiotic foods brings benefits has not yet been sufficiently scientifically proven.
- Drink plenty of fluids: Make sure you drink enough. We recommend 1.5 to 2 liters per day, even more on hot days. Low-calorie drinks such as water, unsweetened teas or fruit juice spritzers are good.
- Make sure you get regular exercise in your everyday life: go for frequent walks or cycle to work. Endurance sports are also considered very healthy: these include cycling, (Nordic) walking and swimming. Exercise gets the bowels moving.
Conservative therapy
The treatment doctors choose for diverticulitis depends on the extent and severity of the disease. It can be uncomplicated (in the majority of cases) or complicated. The therapy is aimed at preventing complications due to inflammation, alleviating acute or chronic symptoms and preventing the disease from recurring. The following treatments are generally possible for diverticulitis:
- Gentle food that does not further strain the bowel, for example water, tea, porridge or soup. If you have acute diverticulitis, it is better to avoid fiber-rich foods such as raw vegetables, whole grain products or flatulent foods such as legumes. Once the symptoms subside, you can gradually switch back to a high-fiber diet. If you have severe diverticulitis, do not eat anything at first. In this case, you will receive all the important nutrients via an infusion.
- Antibiotics (as tablets) if bacteria are involved in the diverticulitis (antibiotics are ineffective against viruses). In severe cases, treatment in hospital is necessary. They then receive the antibiotics in high doses via an infusion.
- Antispasmodic medication (spasmolytics) for cramp-like pain
Diverticular bleeding
Diverticular bleeding is a complication. It can occur as a result of diverticulitis and is one of the most common causes of intestinal bleeding in older patients. If the bleeding diverticulum can be identified (by colonoscopy or X-ray examination), the affected segment of the colon usually has to be removed in an emergency operation.
Surgery
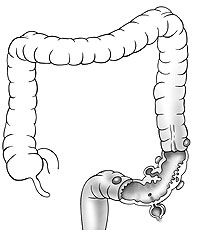
Removal of the sigmoid colon (sigmoidectomy) – In the vast majority of cases, the so-called “sigmoid colon” is mainly affected by the inflammation and should therefore be removed (sigmoid resection). The removal of the sigmoid colon has no disadvantages for the patient. The functions of this intestinal section are taken over by the neighboring intestinal sections. We perform the removal in a non-inflamed state (6 to 8 weeks after an episode of diverticulitis) in the form of a minimally invasive colon removal (“keyhole surgery”, laparoscopic colon segment removal). A camera is inserted into the abdominal cavity through a small incision (2 cm) at the navel. With the help of other fine instruments, which are inserted through small skin incisions (0.5-1.5 cm) in the middle and lower abdomen, the affected section of colon can be detached in the abdomen and then removed through a 7 to 10 cm incision in the lower abdomen. The remaining intestinal ends are then reconnected (anastomosis). An artificial anus is not necessary for this operation. The advantage of the minimally invasive technique is that recovery after the operation is significantly faster and the cosmetic result is better due to the small wounds. As a further therapy, we recommend that patients follow a high-fiber diet.
Laparoscopic sigmoid resection for diverticulosis
- Preparation: small enema
- Anesthesia: General anesthesia
- Operation duration: 120 to 240 minutes
- Hospitalization: 5 to 7 days
- Incapacity to work: 3 to 4 weeks
- Aftercare: no suture removal
- Follow-up: to discuss the histology
Open sigmoid resection for complicated diverticulitis
- Preparation: Emergency operation
- Anesthesia: General anesthesia
- Operation duration: 120 to 240 minutes
- Hospitalization: 7 to 10 days
- Incapacity to work: 3 to 4 weeks
- Aftercare: Suture removal after 10 days
- Follow-up: Stoma consultation
Closure of artificial small bowel outlet (ileostomy repositioning)
- Preparation: none
- Anesthesia: General anesthesia
- Operation duration: 60 to 90 minutes
- Hospitalization: 4 to 5 days
- Incapacity to work: 2 to 3 weeks
- Aftercare: no suture removal
- Follow-up: after 6 weeks
Closure of artificial colon outlet (descendorectostomy)
- Preparation: small enema
- Anesthesia: General anesthesia
- Operation duration: 120 to 180 minutes
- Hospitalization: 7 to 10 days
- Incapacity to work: 4 to 6 weeks
- Aftercare: no suture removal
- Follow-up: after 6 weeks
Emergency surgery for diverticulitis with peritonitis
Emergency surgery is necessary in all cases of severe peritonitis. The affected section of colon is removed through a large incision extending from the middle abdomen to the lower abdomen and stool and pus residues are flushed out of the abdominal cavity. If the remaining intestinal ends are free of inflammation, they can be reconnected with a stapling instrument. Sometimes an upstream artificial anus has to be inserted to allow the new connection to heal. The artificial small bowel outlet in the right lower abdomen is closed again in a second minor operation 6 to 12 weeks after the first operation.
If the inflammation is already so advanced that it is no longer possible to bring the ends of the colon directly together, one end of the colon is closed in the pelvis and the end that passes stool is used as an artificial anus in the lower left abdomen (Hartmann operation). A reunion of the colon with the rectum can be considered again after the inflammation has completely subsided, at the earliest 8 to 12 weeks later.