Conservative measures
Acute anal fissure resolves on its own in rare cases, but usually requires therapy. If doctors treat the tear in time, anal fissure is easily curable. The following options are available for the treatment of anal fissure:
- Pain-relieving medication in the form of ointments, suppositories or anal tampons. The latter are suppositories with a mullein insert that release the active ingredient exactly at the sore spot.
- Muscle-relaxing drugs: Doctors often use ointments containing glycerol trinitrate or so-called calcium antagonists. The active ingredients ensure that the sphincter muscle relaxes. The anal fissure heals better because there is less pressure on it.
- Warm sitz bath: Many people with anal fissure find this pleasant. They relax the sphincter muscle and thus also protect against constipation.
- Diet: Consume plenty of fiber and drink enough fluids. The stool becomes soft, you do not have to push during defecation and thus prevent further tears.
- Botox: Botulinum toxin is a neurotoxin that prevents muscle contraction and causes paralysis. Doctors can inject it into the sphincter muscle that is in spasm, relaxing it. Then the anal fissure can heal better. However, there is a risk of temporary fecal incontinence.
Surgical therapies
Sometimes these non-surgical (conservative) measures are not enough to make the anal fissure heal. Surgical therapy is then the treatment of choice for chronic fissures. Various operations are used to treat chronic fissures.
Internal sphincterotomy (lateral sphincterotomy)
This operation has long been the standard in the treatment of chronic fissures. The partial transection of the internal sphincter muscle, first described by Dr. Eisenhammer in 1951, aims to interrupt the sphincter spasm. Although this surgical procedure has produced very good results and very few relapses, its effectiveness should be weighed against the risk of permanent fecal incontinence. Recent data show an incontinence rate for stool of 20 to 30% of cases. Incontinence typically only becomes apparent 10-20 years after the operation. In our opinion, this operation should only be performed if other surgical procedures have proved ineffective. In this case, however, the sphincter muscle should be cut very sparingly (only about 5 mm of the sphincter muscle should be cut). This operation is only performed at our clinic in exceptional cases.
After an operation, follow-up care is sometimes necessary. Because surgeons do not suture the wound, you must take good care of it. Ointment dressings, for example, are suitable for this purpose. Warm sitz baths can also speed up the healing process. They promote blood circulation and relax the muscles. Bath additives such as camomile may also have a healing effect – but you should discuss this with your doctor first. It is also advisable to gently clean the anus area with water after a bowel movement. Toilet paper irritates the wound and it heals less well. You should allow several weeks for the wound to heal.
Fissure cleaning (fissure debridement)
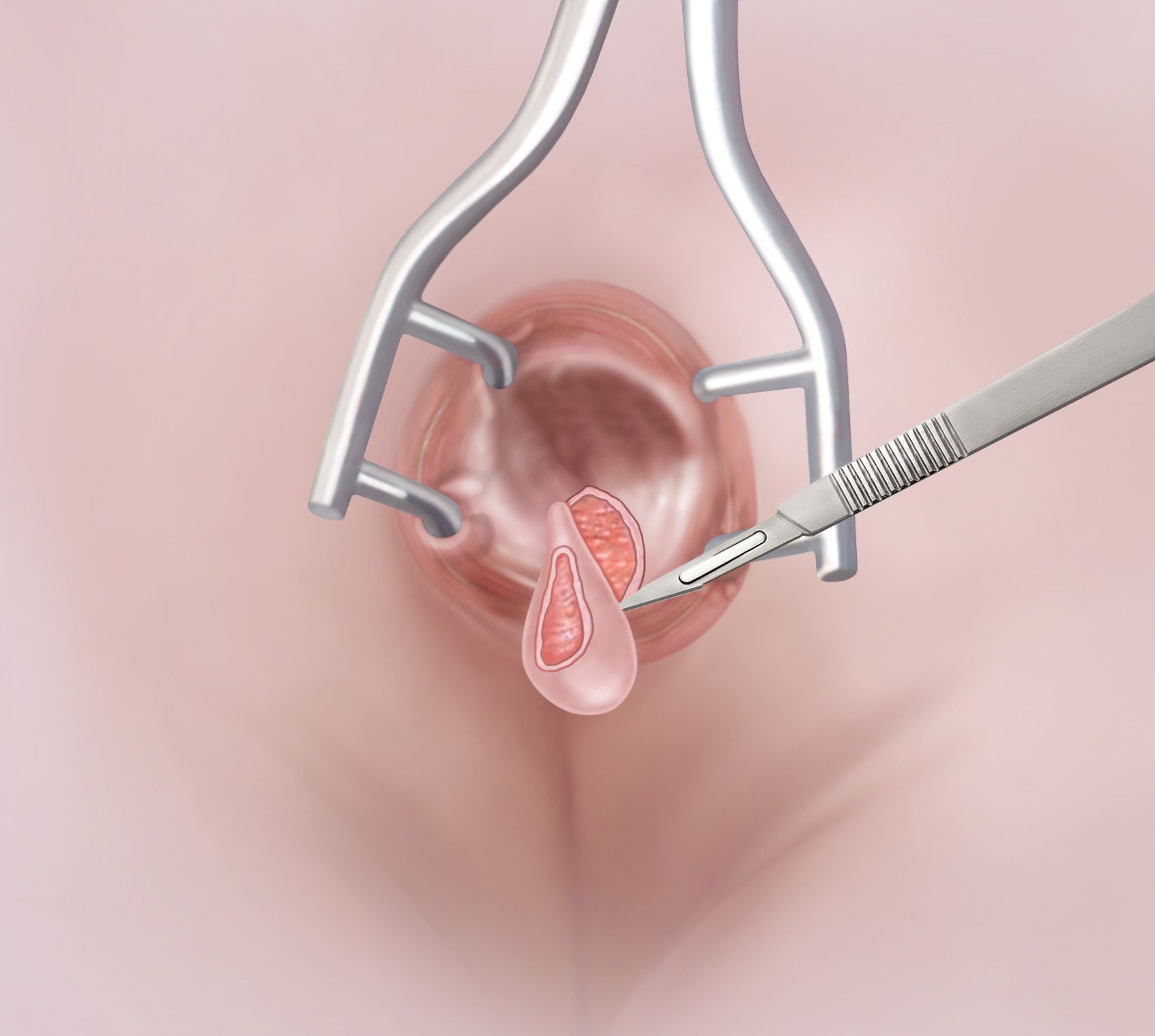
Fissure cleaning with removal of the fissure edges
The aim of fissure cleaning or fissure debridement is to remove all factors that could hinder the healing of the fissure. These include the presence of scar tissue, the usually present sentinel mariscus at the outer end and the enlarged anal papilla at the inner end of the fissure. It is important to cut the edges of the fissure outwards towards the skin so that an outward-facing wound (in the skin) is created. This so-called drainage triangle allows wound secretions to drain away from the surgical site or fissure to the outside. This is a decisive factor for wound healing. This triangle should be large enough, usually about 1-2 cm. The wound usually heals completely in 4 to 6 weeks. Fissure debridement is the treatment of choice in our clinic for the treatment of chronic fissures.
Covering the fissure with a skin flap (V-Y flap)
The V-Y flap is a covering of the tear with a small flap of skin from the anal region. At our clinic, we usually perform this operation after a fissure debridement that has not healed the fissure. With this treatment, it is crucial that there is a soft bowel movement after the operation. Therefore, the intake of stool-regulating agents (psyllium seeds: e.g. Metamucil® 1-3 coffee spoons/day) and mild laxatives (Movicol® sachets 1-2/day, alternatively Transipeg forte® 1-3 sachets/day) is available after the operation.
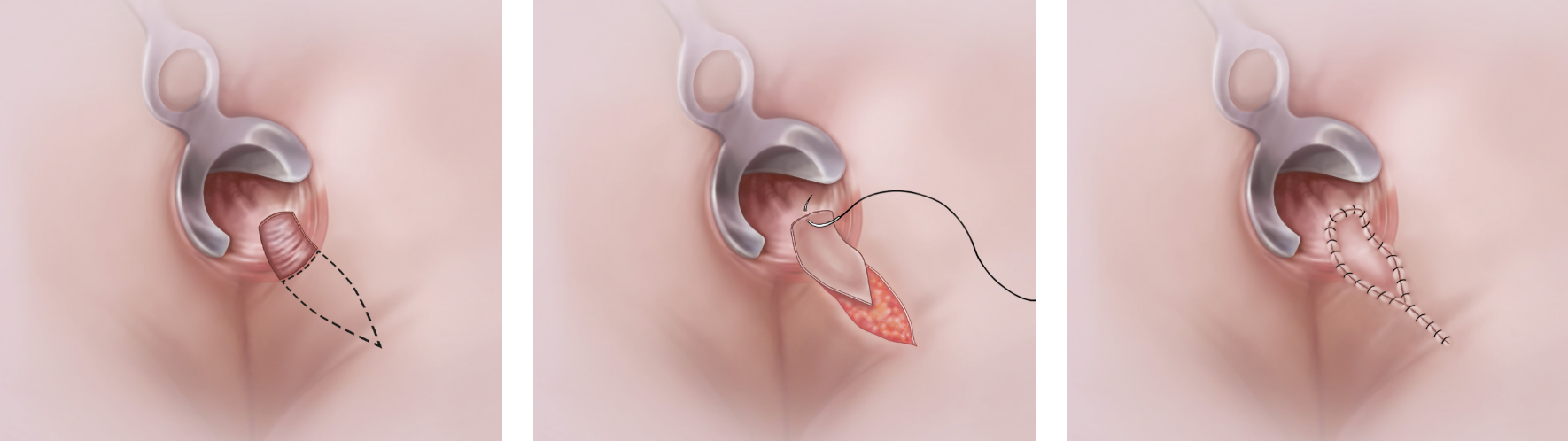
V-Y flap: Covering a tear with a skin flap
Operation information
Fissure cleaning
- Preparation: small enema
- Anesthesia: general anesthesia or spinal anesthesia
- Operation duration: 30 minutes
- Hospitalization: outpatient
- Incapacity for work: 3 to 7 days
- Follow-up treatment: open wound treatment (showering for 2 to 3 weeks)
V-Y Flap
- Preparation: small enema
- Anesthesia: general anesthesia or spinal anesthesia
- Operation duration: 45 minutes
- Hospitalization: 1 to 2 days
- Incapacity for work: 7 to 10 days
- Follow-up treatment: stool regulation