Open surgical and endovascular therapy of abdominal angina
Angina abdominalis (or angina intestinalis) refers to a chronic circulatory disorder of the intestinal wall (chronic mesenteric ischemia). It is an early symptom and is a warning sign of impending occlusion of a vessel supplying the intestine.
Overview
It usually occurs about 20-30 minutes after eating and lasts about one to two hours. The character of the pain can vary from dull to sharp. Food intake causes the stomach and intestinal wall to stretch. The stretching is transferred to the vessels and increases the resistance to blood flow. The consequences are reduced blood circulation and the development of pain attacks. The most common cause is arteriosclerosis of the mesenteric vessels (superior mesenteric artery, inferior mesenteric artery). The risk factors therefore also include arteriosclerosis:
Smoking
High blood pressure
High blood fats
Family history
Procedure
If a chronic circulatory disorder is suspected, it is first necessary to visualize the intestinal vessels. Duplex sonography (ultrasound) is usually the first choice. If the circulatory disorder is confirmed, a computer tomography scan is performed for a detailed assessment. Magnetic resonance imaging can be considered as an alternative. The results are discussed on an interdisciplinary basis and a treatment plan is proposed to the patient.
Open surgical treatment
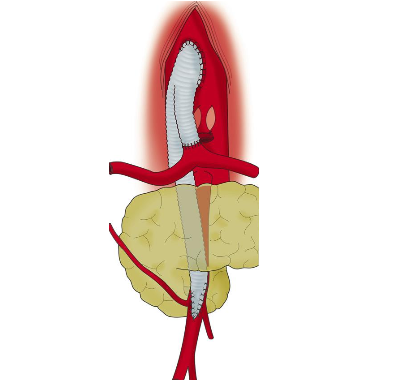
The main artery (aorta) and the affected vessel are visualized via an access through the abdominal wall. The appropriate surgical technique is then used: repositioning of the vessel (replantation/transplantation), creation of a bypass circuit (antegrade or retrograde bypass), reconstruction using a prosthesis (see image) or removal of calcium deposits (thrombendarterioectomy) with vessel dilation (patchplasty).
Endovascular treatment
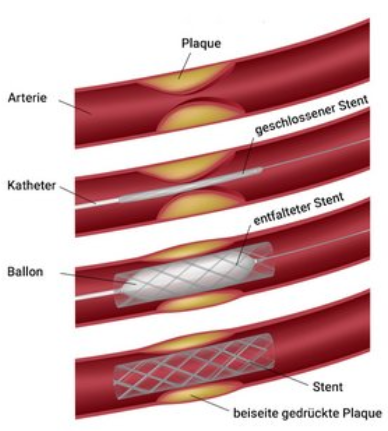
A catheter is inserted into the vessel via a small vascular access (puncture). The constriction is then widened with a balloon. Current recommendations of the specialist associations provide for additional stent implantation. If treatment is necessary, the patient’s situation and the results of the various methods should be considered in relation to each other: Open surgery shows better long-term results overall. Catheter-based interventions have advantages in the short term after treatment. Open surgery would therefore be recommended for younger and otherwise healthy patients. Catheter-based procedures can be considered for older patients and patients with severe secondary diseases. In many cases, both methods complement each other.
Jimenez et al J Vasc Surg 2002
Alila Medical Media / fotolia
Preparation
Special preparation by the patient is not feasible. Treatment of risk factors (e.g., smoking, high blood pressure, etc.) is necessary during and after therapy.
Aftercare
Aftercare depends on the selected therapeutic option (open surgery versus catheter-guided treatment), and may be organized in a special rehabilitation clinic after treatment, if desired. Regular consultations are furthermore arranged in the vascular surgery outpatient department for monitoring of therapeutic outcomes. A change and modification of medication is necessary depending on the procedure performed.
Various procedures at the University Hospital Zurich
Treatment at the University Hospital Zurich offers various advantages. All known and modern treatment methods are available, as are combinations of two methods (hybrid methods) for suitable patients (e.g., ROMS Retrograde open mesenteric stenting). Patients with comorbidities also benefit from the interdisciplinary teamwork of the 43 departments of the University Hospital Zurich.
For patients
As a patient, you can also register directly for an initial consultation. Ideally, you should be referred to us by your general practitioner or specialist. Unfortunately, patients who are insured under a family doctor model cannot refer themselves.