Diagnostics
In the case of a unilateral pneumothorax, the affected side is less well ventilated, resulting in an asymmetrical breathing movement and the chest does not expand evenly. During auscultation, no or only very faint breath sounds are audible on the corresponding side. During percussion, a hollow tapping sound, a so-called nesting sound, is noticeable. However, percussion should always be carried out in lateral comparison with the other side of the thorax. The imaging diagnosis of choice, which usually reliably detects a pneumothorax, is the chest X-ray. As standard, this should be carried out in a standing position and in an inspiratory position in two planes.
The pneumothorax is recognizable here in the sense of a missing vascular pattern. Ultrasound is increasingly being used as an alternative method that can detect even small pneumothoraces quickly, reliably and without radiation exposure. In the event of a recurrence (repeated occurrence) of a pneumothorax and if an underlying disease of the lung (secondary pneumothorax) is suspected, a computer tomography (CT) scan should be performed to identify any underlying concomitant injuries or diseases.
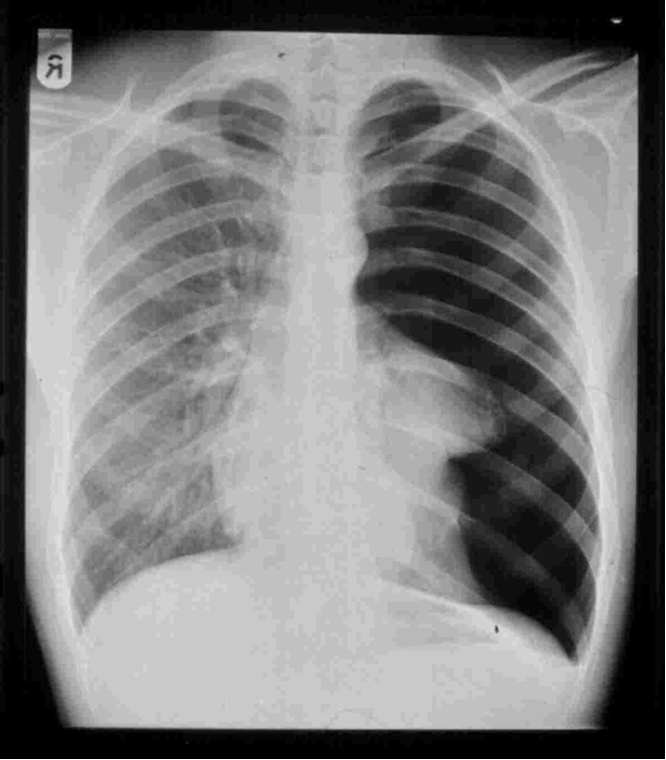
Total collapse of the left side of the lung in the sense of a pneumothorax in a standing X-ray using the a.p. technique.
Therapy
If it is an idiopathic spontaneous pneumothorax and occurs for the first time, it is usually treated conservatively.
Conservative treatment consists of close monitoring of the course of the X-ray in the case of minor spontaneous pneumothorax. However, the decision should be made in close consideration of the clinical symptoms. In all other cases, a so-called thoracic drain is inserted so that the negative pressure within the thorax is restored and the lungs expand.
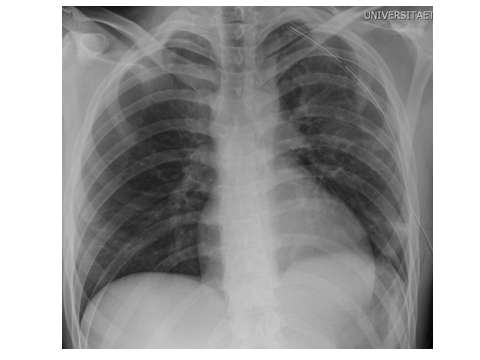
Complete expansion of the left lung after insertion of a chest tube.
If the pneumothorax is traumatic and there are other injuries such as rib fractures or a hemothorax (blood in the pleural cavity), a chest tube must always be inserted to drain the pneumothorax and any abnormal fluids such as blood or other effusion. In the case of a tension pneumothorax, there is a maximum emergency indication and the drainage must be inserted immediately.
Surgical intervention is often recommended in the event of a recurrence of a pneumothorax (repeated occurrence), persistent air loss over 3-4 days or in the presence of a secondary pneumothorax (i.e. a lung disease). This involves a thoracoscopy of the affected chest cavity under general anesthesia. In order to close the leak in the pleura, a sparing wedge resection is performed in the affected section of the lung, usually in the apex area. In addition, a so-called abrasion of the pleura, i.e. a roughening of the lung to adhere it to the chest wall, is performed. In certain cases of recurrence of pneumothorax, talc pleurodesis, a bonding of both skins using talcum powder, is performed.