The main symptoms of this clinical picture are shortness of breath on exertion and later also at rest (dyspnea), a feeling of tightness in the chest(angina pectoris) and/or fainting (syncope).
Preparation
The following preparatory examinations are necessary: Cardiac ultrasound (echocardiography), cardiac catheter diagnostics with visualization of the coronary vessels and, if necessary, measurement of the pressure values in the pulmonary circulation, computer tomography with visualization of the heart and the access vessels.
Procedure
The procedure is usually performed under local anesthesia; general anesthesia is not usually necessary. The biological heart valve “folded” onto a catheter system is positioned and released into the narrowed and calcified aortic valve via the femoral artery and the aorta under X-ray fluoroscopy. The blood flow over the heart valve is minimized during valve release by rapid stimulation of the heart via a temporarily inserted pacemaker probe. A basic distinction is made between balloon-expandable and self-expanding flap systems. The optimum individual system is selected based on the anatomical conditions. The catheter system is then removed and the puncture sites in the area of the access vessels are sutured. The procedure takes approx. 30-60 minutes.
This procedure can also be used to treat patients with worn (degenerated) biological heart valves following surgical replacement of the aortic or mitral valve (see valve-in-valve therapy).
Patients with narrowed leg arteries can be treated via alternative access routes. In addition to the surgical access options via the apex of the heart, via the aorta or via the subclavian artery, a gentle access via the leg vein (transcaval access) has been established at our clinic as a safe minimally invasive alternative. For patients who are particularly at risk, we use special methods such as the BASILICA technique to prevent blockage of the coronary arteries and thus a heart attack. We also use protection systems to prevent strokes in patients at increased risk.
Balloon dilatation of the aortic valve (aortic valve balloon valvuloplasty) is often performed in preparation for TAVI, but is now rarely performed as the sole procedure.
After the procedure
After the intervention, monitoring is necessary for at least twelve hours, and bed rest with a pressure bandage should be maintained for about six hours. In total, an inpatient stay of at least two nights must be expected for the procedure.
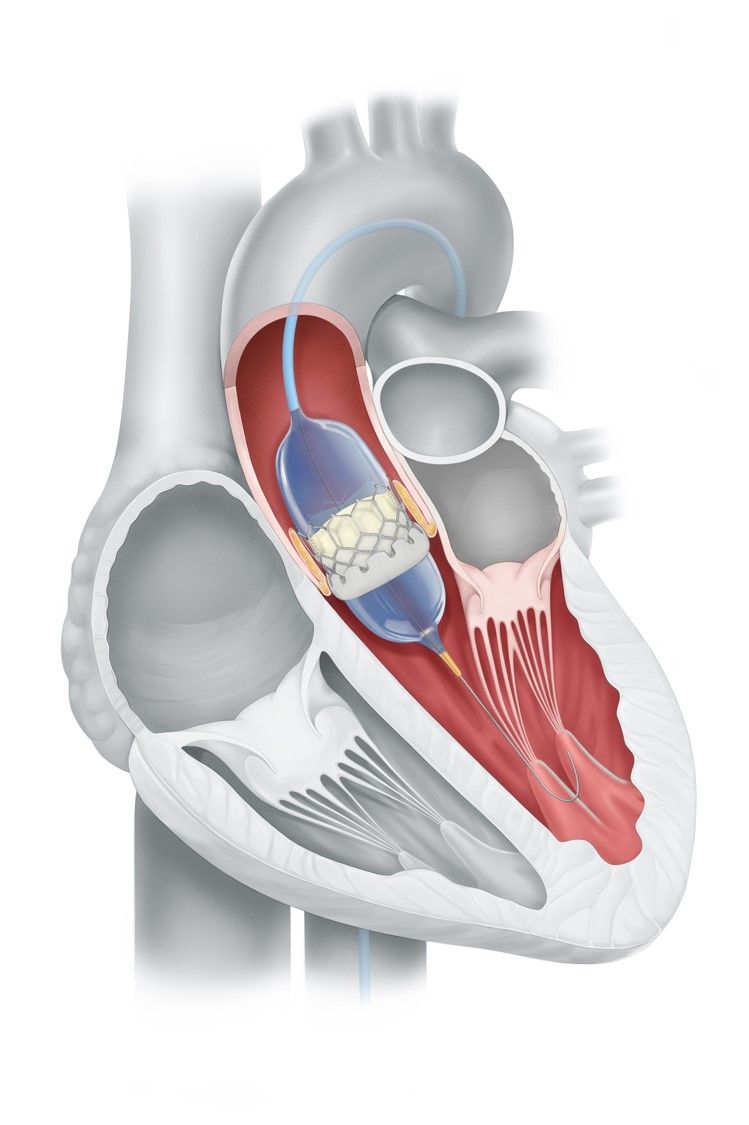 TAVI: Implantation of a biological catheter valve in the area of the narrowed aortic valve using a balloon catheter system.
TAVI: Implantation of a biological catheter valve in the area of the narrowed aortic valve using a balloon catheter system.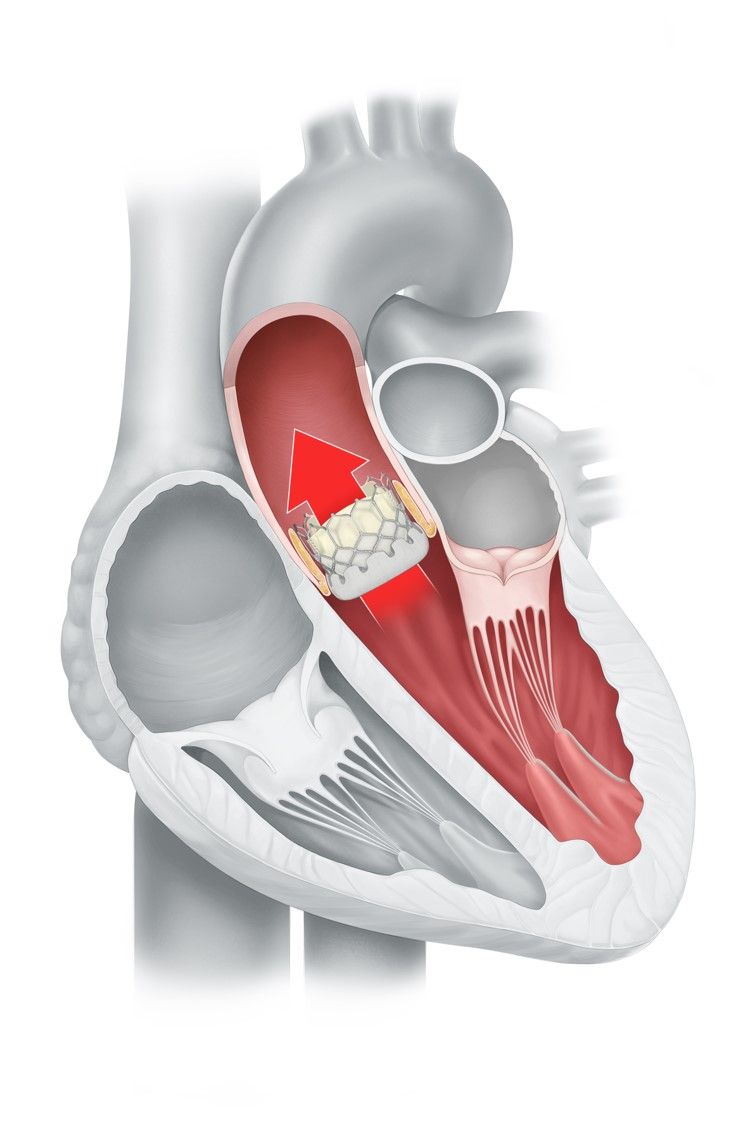 After TAVI: Biological aortic valve in position with normal blood flow from the left ventricle to the aorta.
After TAVI: Biological aortic valve in position with normal blood flow from the left ventricle to the aorta.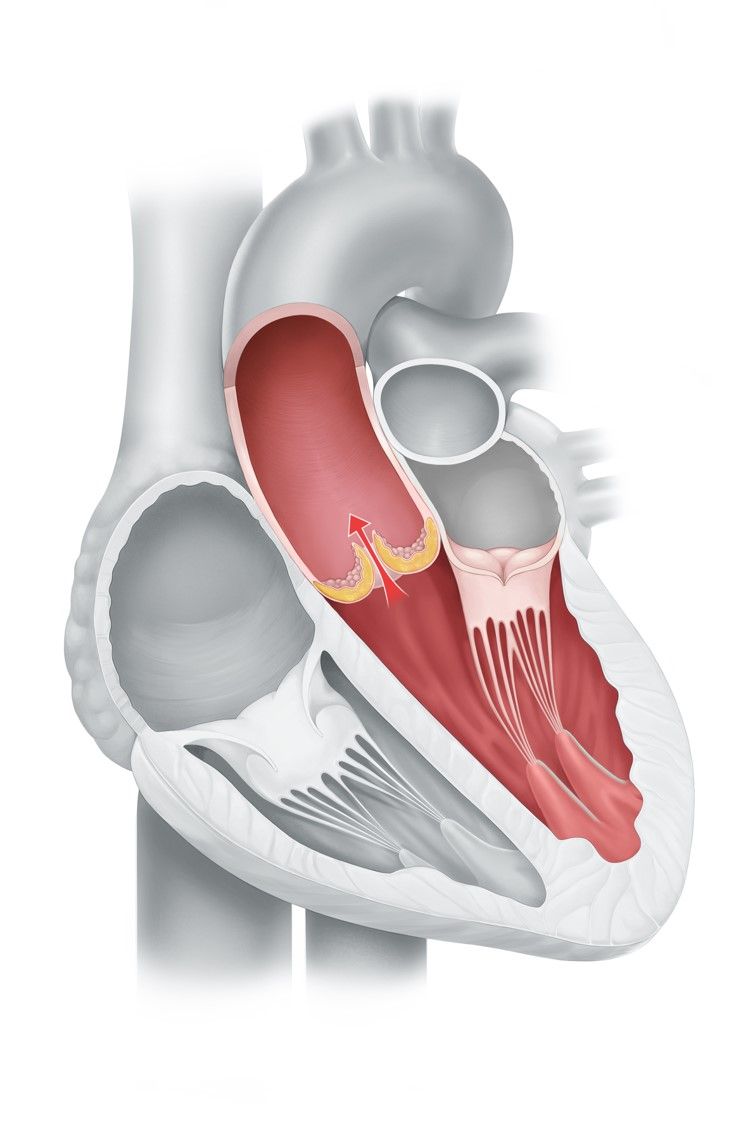 Before TAVI: Severe aortic valve stenosis, the blood flow from the left ventricle towards the aorta is significantly impaired.
Before TAVI: Severe aortic valve stenosis, the blood flow from the left ventricle towards the aorta is significantly impaired.

