Procedure
This increases the predictability with regard to the desired surgical goal and the safety of the surgical procedure and negative postoperative “surprises” can be avoided. Surgical procedures in the head and neck area require in-depth knowledge of the anatomical structures. In the cranial region in particular, functionally and aesthetically important structures come together in a very confined space. Restoring the correct occlusion in trauma affecting the upper and lower jaw is a particular challenge for oral and maxillofacial surgeons. In addition to the clinical examination, which remains indispensable, imaging procedures can also reveal even the smallest changes in the anatomical conditions preoperatively. Two-dimensional procedures such as conventional X-ray diagnostics are used for uncomplicated mandibular fractures, for example. However, as they are very limited due to the superimposition of structures, modern surgical planning systems based on three-dimensional computer or digital volume tomography represent the standard in our clinic for the diagnosis and treatment of complex craniofacial trauma and for secondary reconstruction of fractures that have healed in a malposition.
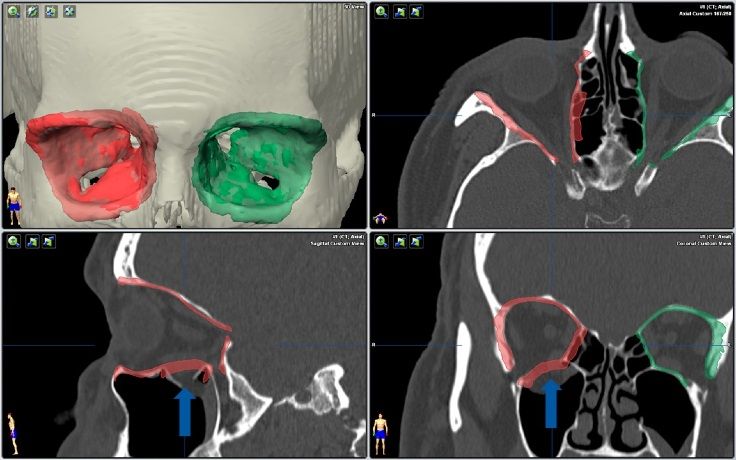
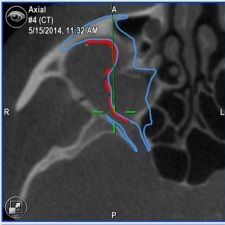
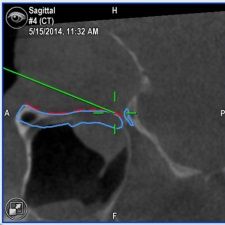
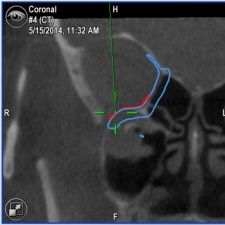
Secondary surgery of a right orbit, preoperative planning. The non-fractured right side (green) is mirrored onto the affected fractured side (red) to create a virtual template. The orbital floor fracture is marked with a blue arrow.
Digital data processing allows detailed insights into bone and soft tissue to be obtained from a single image data set without additional radiation exposure. In addition to automatic segmentation and mirroring of individual sections of the three-dimensional data sets, it is also possible to freely shift and deform the segments and import CAD (computer-aided design) data sets for the simulation of any preformed three-dimensional objects (e.g. titanium implants for the reconstruction of individual structures of the facial skull). This means that bone and implant-based reconstructions as well as bone-displacing operations can be performed virtually. The patient-specific implants can either be produced indirectly on preoperatively created patient models or directly laser-sintered.