The treatment is aimed at people who suffer from chronic facial pain. You will receive an overview of the various causes of pain and the respective treatment options.
Overview
Neuropathic pain occurs when the pain-conducting nervous system itself is damaged and no longer transmits impulses correctly.
Chronic neuropathic pain syndromes are among the greatest challenges in neuromedicine. Trigeminal neuralgia is one of these syndromes. It leads to a flash of pain in the face, often described as electrifying, which is triggered spontaneously or by causes such as a draught, touch, talking, brushing teeth or eating. Although the pain only lasts for a moment or a few seconds, it easily reaches the maximum level of pain imaginable for humans. Typically, only one side of the face is affected, especially the cheek or chin area. It can also happen that the pain disappears completely for months and then returns in its familiar form.
In Switzerland, around 500 women and 350 men over the age of 40 are newly affected each year. A distinction is made between the syndromes according to the cause of the pain. In some patients, a cause is found using modern imaging techniques and is then referred to as “typical trigeminal neuralgia”: close to the brain stem, where the trigeminal nerve enters the pons, a blood vessel, usually a loop of the superior cerebellar artery, is in contact with the nerve. That in itself is not pathological. Close contacts between nerves and blood vessels occur everywhere in the body. In unfortunate cases, however, the constant pressure on the nerves leads to demyelination. This is a weakening of the myelin sheaths, which surround each individual nerve fiber like insulation. This results in the unintentional skipping of electrical impulses from sensitive fibers to pain fibers. At any rate, this is how the cause of the disease is nowadays imagined in very simplified terms.
In other cases, no such conflict is found and these are therefore referred to as “idiopathic trigeminal neuralgia”.
There are also a myriad of other diseases that can also lead to very similar facial pain. These include tumors, strokes, demyelination in multiple sclerosis and viral diseases such as herpes zoster. And last but not least, dental and jaw diseases can of course be responsible for the pain. The dentist is therefore often consulted first. It is not uncommon for multiple dental treatments and extractions to precede a referral to a neuromedical specialist. An early magnetic resonance imaging scan for attack-like electrifying facial pain can shorten the patient’s suffering.
Forms of treatment
There are various treatment options. They differ according to the cause of the pain.
Drug treatment
If no curative therapy is available, such as in the case of a brain tumor that can be surgically removed, it is always worth trying to treat it with medication, which is usually successful. The drugs used mostly come from the group of antiepileptic drugs, have a membrane-stabilizing effect and thus raise the stimulation threshold for the pain fibres of the trigeminal nerve.
The medication carmamazepine or alternatively oxcarbazepine is gradually increased in dosage, provided it is well tolerated and does not impair the patient too much due to drowsiness. Lamotrigine, gabapentin, phenytoin and other drugs are also used.
The time for interventional treatment
Escalation therapies are only used if drug therapy is not sufficiently effective, medication is not tolerated or the side effects are intolerable for the patient. The treatment can follow three different approaches.
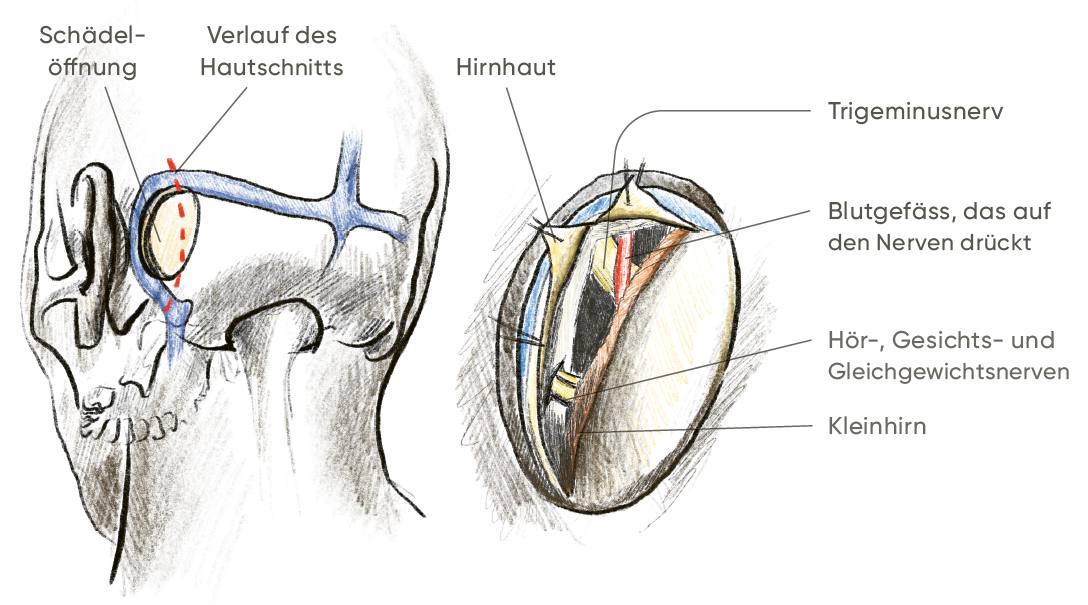
Microvascular decompression eliminates the cause of typical trigeminal neuralgia, the conflict between nerve and blood vessel.
If this is not possible or not successful, ablative procedures are used. This involves the targeted destruction of nerve fibers, either with X-rays, pressure, heat or chemicals.
The final escalation stage is the possibility of neuromodulation. These procedures may only be used after all alternatives have been exhausted and following a joint decision by experts from different disciplines.
This alters the perception of pain in the brain itself: The pain is usually combated through the use of “brain pacemakers”.
1. microvascular decompression according to Jannetta
From a neurosurgical point of view, this treatment is ideal, although it represents the largest surgical intervention of the alternatives listed.
Procedure
After anesthesia, the skull is opened via a skin incision just behind the ear. A “window” about the size of a two-franc ring is sufficient for this. Under the surgical microscope, a path is then followed between the bone of the petrous bone and the cerebellum without damaging any tissue. Using fine micro-instruments, the blood vessel is carefully detached from the nerve and pushed away. To prevent the nerve from falling back into its old position, a small sponge made of Teflon fibers is placed between the nerve and the blood vessel.
Opportunities and risks
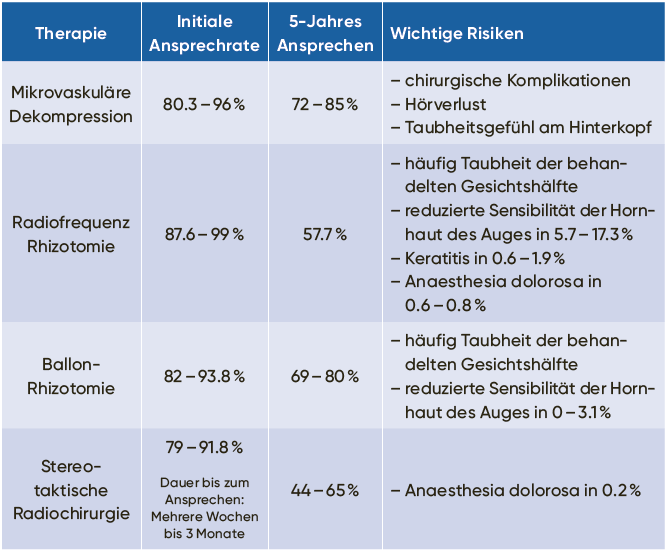
The procedure results in immediate pain relief in 80 to 96 percent of cases. Between 72 and 85 percent of patients are still pain-free five years after the procedure and do not require any medication.
Side effects
Common: localized numbness at the back of the head above the surgical scar; temporary pain in the surgical area; temporary dizziness and nausea.
Rarely: Complications such as hearing loss, hearing loss on the treated side or loss of sensation in the face.
Very rare: serious complications such as wound infection or cerebral hemorrhage. The latter can even be life-threatening.
The decisive advantage of this procedure is that the brain and the nerves themselves are spared.
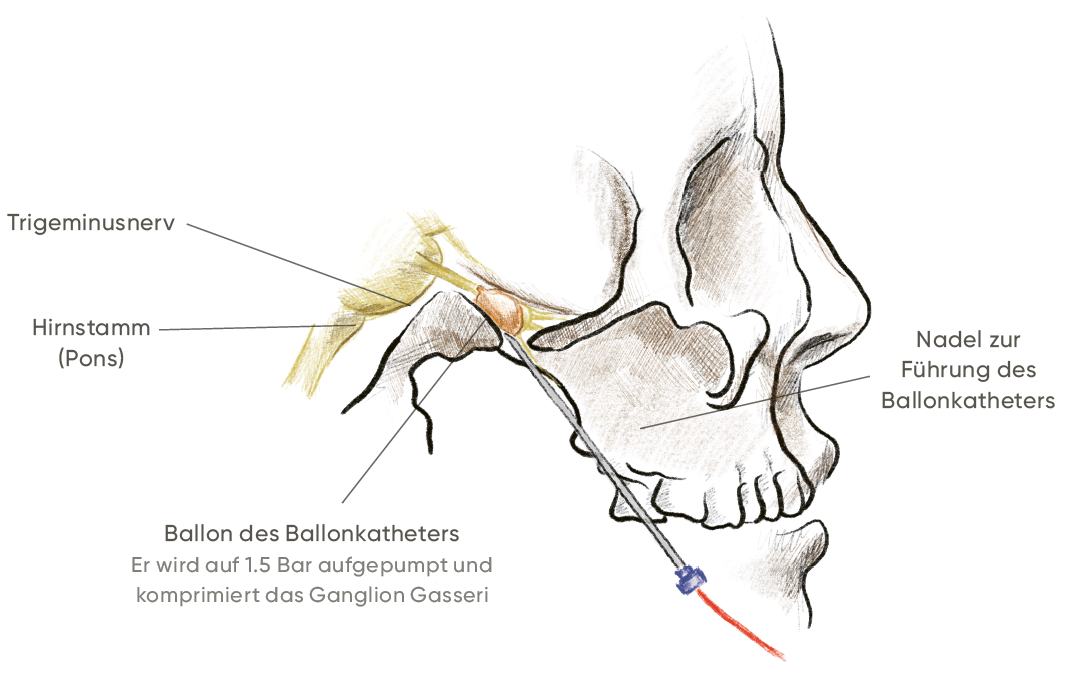
2. rhizotomy of the ganglion gasseri
We choose an ablative procedure, i.e. a “tissue-destroying” procedure, in the following cases:
If no vascular-nerve conflict is recognizable in the imaging.
If microvascular decompression was not successful.
If a major operation is to be avoided due to the patient’s individual risks, such as advanced age, or if the patient does not wish to undergo such an operation after weighing up the risks and burdens.
Procedure
In a rhizotomy of the ganglion gasseri, a needle is used to puncture the foramen ovale at the base of the skull either from the corner of the mouth or directly through the oral cavity. The needle is then used to damage the ganglion gasseri (the part of the facial nerve where it divides into its three branches) in its connective tissue space, the cavum Meckeli, through the foramen ovale. This is done either by introducing an alcoholic solution (glycerol filtration), by heat (radiofrequency ablation according to Sweet) or by pressure (balloon compression).
Opportunities and risks
Various studies have examined the prospects of success and risks of the procedures. However, only a few of them have checked these and even fewer have systematically compared the different methods. Nevertheless, it can be said that initial success can be expected in around 80 to 100 percent of cases. Around 60 to 80 percent of patients are still pain-free after five years.
Side effects
Frequent: temporary numbness in the face
Rare: a permanent feeling of numbness in the face
Very rare: other complications
The most serious complications include
the “anesthesia dolorosa”. This is a complete numbness of the face accompanied by pain.
Blindness due to damage to the cornea. This occurs when the eye is numb and its protective reflexes no longer function as usual.
The procedure is comparatively minor and less stressful for the patient, but aims to permanently destroy nerves. Therefore, from the neurosurgeon’s point of view, it is actually “more difficult” than the microvascular decompression mentioned above. However, this procedure is also suitable for patients with other forms of trigeminal neuralgia and neuropathy, such as facial pain in multiple sclerosis or when no cause can be identified.
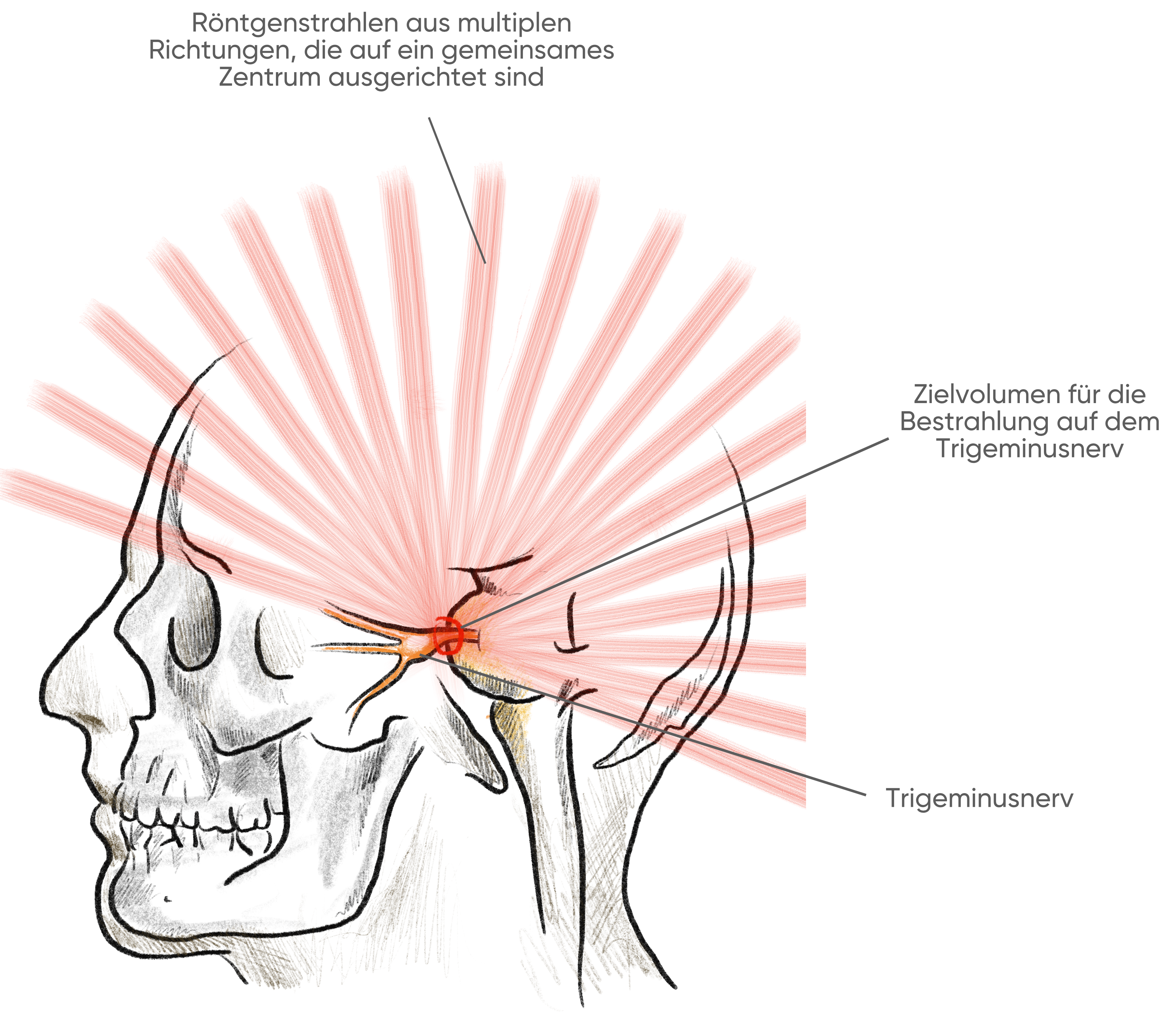
3 Radiosurgical treatment
Radiosurgery is even less stressful than the procedures listed above. The principle is the same as with the other ablations: Pain-conducting nerves are destroyed in a targeted manner, thereby relieving pain. This is achieved by single-stage stereotactic irradiation of the trigeminal nerve with a very high radiation dose of 70 to 80 gray, whereby the distance to the brain stem is chosen so that it receives less than 20 gray of radiation. The entire treatment is possible in one day – unlike radiotherapy for most tumors.
Opportunities and risks
This form of treatment is possible without anesthesia. Any blood thinning does not have to be interrupted for this. However, the pain-relieving effect only occurs after several weeks. In addition, comparative studies have shown that the chances of success are not quite as good as with the other procedures, at 92 to 97 percent initially and only 44 to 65 percent after five years.
The risk of permanent facial numbness after treatment is around 20 percent. The advantage of this is that the surgical risks, most of the stresses and strains and the hospital stay are eliminated.
The procedure is a good alternative to rhizotomy and is particularly suitable for patients with contraindications to surgery.
4. neuromodulation
The final treatment option is neuromodulation.
The most important of these is deep brain stimulation. As already mentioned, these procedures are not part of standard therapy and are therefore only used in individual cases after careful consideration and after treatment alternatives have been ruled out.
Peripheral nerve field stimulation
It is an elegant form of neuromodulation.
Procedure
During this surgical procedure, we implant fine electrodes under anesthesia into the areas of skin affected by pain. The electrodes are connected under the skin to a pacemaker (comparable to a heart pacemaker) so that they are not visible from the outside. The electrical field built up in the skin in this way is perceived as a tingling sensation or warmth and, according to the gate control theory, overlays the pain.
In very simplified terms, this theory states that the inputs for pain information to the central nervous system firstly have a limited capacity
and secondly, are controlled by gate mechanisms that can be opened and closed by the central nervous system. Alternative stimuli can be used to specifically reduce the permeability of these “gates”. Everyone knows this instinctively: rubbing an injured area of skin can help to reduce the sensation of pain. Many neuromodulation methods are based on this principle. They reduce the pain stimuli transmitted to the brain by closing these gates with electrical impulses.
Opportunities and risks
This procedure is particularly attractive because the entire procedure takes place only in and under the skin. This means that apart from a low risk of infection and wound healing disorders, no complications are actually to be expected. There is no reliable data on the chances of success, but in our experience at the University Hospital Zurich, this treatment is well suited for patients with facial pain following zoster ophthalmicus.
Today, deep brain stimulation is used in particular to treat Parkinson’s disease, but was originally developed for the treatment of chronic pain.
For a short time, the procedure was approved by the US Food and Drug Administration (FDA), but is no longer approved today. The reason for this is that, to date, there are no studies of sufficient method and scope to prove the effectiveness of the procedure. There is a very wide range of implementation options for this treatment. The electrodes can be implanted either in the posteromedial or posterolateral thalamus, the centromedian thalamus, the periaqueductal gray or the cingulate gyrus. The electrodes are then also connected under the skin to a neurostimulator. This is implanted in the chest or abdominal area in the same way as a pacemaker. In selected cases and when alternative methods have been exhausted, this procedure may be considered after careful interdisciplinary consideration.
Summary
The treatment of chronic facial pain is an interdisciplinary task. The most important thing is that you as a patient are well informed about the various treatment options of the individual medical disciplines. If conservative treatment is not successful, an interdisciplinary board should discuss further treatment where possible.
Comparison of the opportunities and risks of the procedures
External content
Please accept cookies to display this content from an external website.